
I think we all can agree that having an understanding of our equipment and its limitations plays a strong role in our ability to operate smoothly on-scene and deliver the best possible patient care.
Most systems out there now acquire blood pressures using automated cuffs. These are nice because they save us time and limit the repetitive process of placing the cuff, pumping it up, relieving the pressure, and listening with a stethoscope…. They free up our hands to do other things. While they’re nice, they come with their own set of limitations… I think most would agree that these limitations are probably more substantial in the prehospital environment. I want to delve into how a lot of these monitoring devices work.
Out of the three pressures listed below, which one do you think is most accurately measured by the monitor? The systolic, diastolic, or MAP?
If you said the MAP then you’re completely right.
Most noninvasive blood pressure devices use what’s called the oscillometric technique. Instead of picking up sounds like a stethoscope, it’s picking up oscillation amplitudes. Once the external pressure of the cuff exceeds the intra-arterial systolic pressure, arterial blood flow past the cuff ceases. When the pressure from the cuff is released, a pressure sensor begins to detect the arterial pulsations as oscillations. As the pressure within the cuff decreases, the point of max oscillation amplitude is reached. This point of max amplitude represents the MAP which is the only pressure that is directly measured. The computer then uses an algorithm or parameters set in place by the manufacturer to generate the systolic and diastolic values.
Note: we are just covering oscillation devices that measure values on deflation (these are the most common). There are some oscillation devices that measure values on inflation.

Just to refresh, the formula for calculating a MAP is as follows:
2(Diastolic) + Systolic/3
A perfusing MAP is said to be at least 65 mmHg. I don’t think we should view this as a “one size fits all.”
Now check this out…..
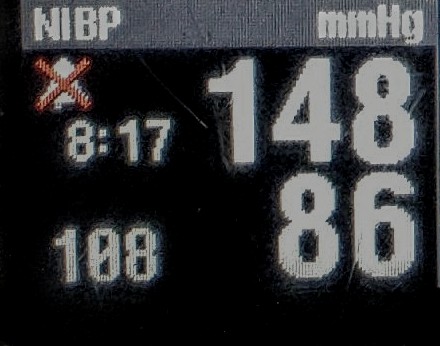
I took several blood pressures this morning using the automated cuff on the cardiac monitor at work. The BP’s were acquired on separate individuals in their 30’s with no known PMH. All of these readings were acquired while sitting stationary with little to no movement. You’ll notice that when we calculate the map using the systolic and diastolic values produced by the monitor, we end up with a different MAP value than what the monitor displays. This is because the monitor is computing the SBP and DBP based off of estimates from the MAP… Its not using the MAP formula we commonly use. Monitoring devices commonly perform this estimation by fixed ratios of the maximal oscillation amplitude. You’ll also see that one person’s BP is reflective of copious amounts of coffee spiked with spoonfuls of diabetes.

Some well-calibrated commercial devices may be pretty valid in regards to calculating oscillometric systolic and diastolic values. However, what’s been most validated is maximal oscillation amplitude accurately corresponding with mean arterial pressure. In my opinion, it seems much more sensible to monitor the directly measured and more validated option.
So, what are some of the factors that can contribute to inaccurate readings? Anything that alters the oscillation amplitude or regularity will produce erroneous results. So… you guessed it… This includes those wonderful and often times not so subtle road vibrations… and of course patient movement. Other things are said to include improper cuff sizing, increased arterial wall stiffness due to arteriosclerosis, and arrythmias. The pictures below were taken from the Zoll X-Series Operator’s Manual. This is no knock on Zoll, this is just to provide you with an example of the limitations one manufacturer recognizes. Pay extra close attention to the first bullet on the second image.


Its important to note that each manufacturer has its own method, meaning there may be considerable variation between machines. This post was meant to provide a brief overview on the technology a lot of us use. Its certainly not specific to any one monitoring device.
Final thoughts….
If you ever doubt the values displayed by your monitor take a manual BP. Technology is great but it’s not always the most accurate option.
.
Follow our social media to stay updated!
https://m.facebook.com/SCOPEeducation20/
https://twitter.com/scopeducation?lang=en
This site is meant to be used for educational use only. We strive to push evidence based medicine with no bias to help you obtain all the important information. You should always follow your protocols that have been set in place.
–Scopeducation Team (Ryan FP-C, CCP-C)
References
https://biomedical-engineering-online.biomedcentral.com/articles/10.1186/1475-925X-11-56
https://acphospitalist.org/archives/2009/10/traps.htm
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3541069/
https://onlinelibrary.wiley.com/doi/full/10.1111/jch.13460
https://www.ahajournals.org/doi/full/10.1161/HYP.0000000000000087