
For you YouTube video:
What exactly is a wide complex tachycardia (WCT)? A WCT is a rhythm with a ventricular rate over 100 bpm and a QRS complex ≥ 120ms (3 small boxes). We’ll be hitting on the following topics:
SVT with Aberrancy VS Ventricular Tachycardia
First off, SVT with aberrancy is just a fancy term that means some type of SVT with some kind of conduction delay such as a right bundle branch block or a left bundle branch block. All health care providers have seen online content trying to differentiate between VT and SVT. You see people arguing about how to diagnose these patients based on a 12 lead ECG. So let me make it super simple with some easy facts:
The most sensitive marker of origin is not the ECG, it’s the patient’s age and whether or not they’ve had any history of heart disease. V-tach accounts for over 80% of wide complex tachycardias. Treat it as V-tach and don’t hesitate to move down the electricity pathway.
Ventricular tachycardia is thought to be a re-entry circuit that circles around scar tissue in the ventricles. A history that includes myocardial infarction makes this more likely to happen.
Here’s some commonly used criteria for diagnosing ventricular tachycardia:
These may be nice and all but let’s go with a more simplified approach:
What is the patient’s age?
Any cardiac history?
Is there any AV dissociation?
And that’s it. If you have an older patient or a patient with a history of MI, you have a high probability of accurately diagnosing ventricular tachycardia. Here’s an example of AV dissociation:

You may be thinking… “Well what about the different formulas and the first set of criteria you brought up? Isn’t that the best system?” The answer is NO. There have been countless studies conducted in an attempt to identify if any caliper driven equation or sign has a high enough specificity and sensitivity to diagnose VT over SVT with aberrancy. NONE are as accurate as the three questions of the more simplified approach. Recent studies say that even if you have a previous 12 lead of the patient showing a LBBB or RBBB you should still assume VT. This is because there are different types of VT that can cause BBB morphologies (below is a video on the subject). So if it is a regular wide complex tachycardia and not 1 big box wide with no P before every QRS, it is VT, or VT, or VT.
Here is some nice philosophy:
Paul Dorion’s philosophy
“We’re all subject to stone age cognition. Our cognitive pathways were designed 500,000 to 2 million years ago. Our cognitive pathways are designed to look for unusual or extraordinary things. That’s how we’ve survived as a species. What we’re left with in an intellectual specialty like medicine. We remember the unusual things, we remember the canaries. We are prone to focus on strange, weird, unusual things. We don’t remember the ordinary things because they’re not memorable. People remember is the 1/20 case that was SVT with aberrancy and they forget the 19/20 times it was V-tach.” The following was a quote from Paul Dorion which was featured in the podcast below:
https://emergencymedicinecases.com/tachydysrhythmias/
VT is exponentially more deadly than SVT. So you will never go wrong with treating the most deadly of the two rhythms first. And the AHA states the safest and most effective way of treating tachycardic rhythms is synchronized cardioversion.

Atrial Fibrillation with Preexcitation (Wolff-Parkinson-White)
I won’t go into to much detail on this because we have a whole post and youtube video that you can check out.
https://scopemeded.com/2020/07/20/the-baby-steps-in-wolff-parkinson-white-syndrome/
So you have a patient with this 12 lead complaining of “just not feeling right”
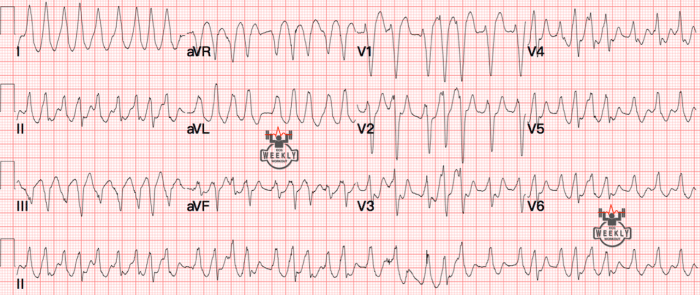
This is a WCT with rates hitting 200-300 BPM. You can see in the precordial leads that this rhythm is irregularly irregular. Only a few tachycardia’s can be irregularly irregular:
But none of these options can hit this fast on their own. There are no P waves so that knocks out MAT. No flutter waves noted (especially in the money lead V1) so that’s out. So what has a high atrial rate and is the only option left? Atrial Fibrillation.
A-fib has a maximum rate of around 180 BPM so the fact it’s hitting 200-300 BPM means there’s an accessory pathway. Even though you can’t see the delta waves in this 12 lead, you can see the different QRS sizes/morphologies which also suggests preexcitation.

What are your treatments for this? Amiodarone? Cardizem? Adenosine? Digoxin? Procainamide? Well only one of these is correct, the others will get you this rhythm:

Procainamide and synchronized cardioversion are the only two acceptable treatments for this rhythm. In the other post and video I go into this rhythm more thoroughly, so check them out if you want to learn more.
Tricyclic Acid (TCA) Overdose
Here are common Tricyclic acids:
•Amitriptyline. •Amoxapine. •Doxepin. •Imipramine (Tofranil) •Nortriptyline (Pamelor) •Protriptyline. Trimipramine.

You have a 26 y/o male found unconscious. Friend’s state that he recently broke up with his girlfriend and was depressed. He was found by family having a seizure. Vitals:
Heart rate: 120+
Respiratory rate: 26
BP: 62/41
BGL and Temperature are normal. No history except depression.
Most often when we do a 12 lead, we pretty much do an 11 lead because most people exclude aVR and consider it a “trash lead”. Well in this case we need this lead to diagnose a TCA OD. Signs on a 12 lead that point towards a TCA OD include:

Or you can do the thumb method!

2. Tall prominent R wave in lead aVR
3. Prolonged QTc (over 500ms)
Now what is our treatment going to be for this patient?
Remember when I said that a prolonged QTc can develop with a TCA overdose? Torsades De Pointes can occur so be ready with Magnesium to combat this dysrhythmia. But the main medication that needs to be given to these patients is our little buddy sodium bicarbonate. In many hospitals, physicians give 100-150 mEq of sodium bicarbonate to TCA overdose patients. Constantly monitor blood gases and electrolytes.

Hyperkalemia
This is one of my favorite topics so this will have its own post that will go into more detail soon.
Is this a regular wide complex tachycardia? Yes and no. This is what the great educator Amal Mattu would call a Regular Really Wide Complex Tachycardia (RRWCT). Look at that QRS! It is pretty much one large box wide. Normal VT does not go that wide. When you see a QRS with the width of one large box, you need to think tox/metabolic. The rate is just over 100 BPM. Ventricular tachycardia (depending on what source you want to use) normally starts at 120 or 130. For the most part, hyperkalemia will not hit that rate (there are of course some exceptions but it is rare).
Hyperkalemia is believed to be a sodium channelopathy. So if you gave any antiarrhythmics (if you mistakenly diagnosed this as VT) such as procainamide, amiodarone, or lidocaine per ACLS, you would send this patient right into ventricular fibrillation because they are sodium channel blockers and you wouldn’t want to give a sodium channel blocker to already poisoned sodium channels would you?
Speaking of misdiagnosing this as ventricular tachycardia, if you start electrically cardioverting these patients you will notice there will be no change in the rhythm and you will develop a low patient satisfaction score.
So before we go into treatment, what are some conditions that can cause a patient to become hyperkalemic?
As you can see, it is important to identify the causes of this deadly electrolyte imbalance. So what’s the treatment for these patients?
Some studies say that using albuterol can cause a slight transient increase in serum potassium prior to it decreasing. In an emergent situation, the number one drug to give these patients is Calcium to stabilize the myocardium and to prevent these patients from going into a ventricular dysrhythmias.

In the hospital, providers may elect to use Kayexalate for non-emergency hyperkalemia. This medication takes hours to days to work.
Recap
3. TCA overdose… Support ABCs and don’t delay on Sodium Bicarbonate
4. Hyperkalemia… look at the width of the QRS complex (one large box, think tox/metabolic) and immediately give calcium. If you encounter difficulty distinguishing between hyperkalemic or in VT, don’t hesitate to give calcium. If the QRS narrows, you know it’s not VT. If nothing occurs, no harm is done and you made their bones stronger. Don’t hesitate to repeat calcium administration.
Follow us on Social Media so you can see when we post!
https://www.facebook.com/pages/category/Education-Website/SCOPE-Education-105632557828024
This site is meant to be used for educational use only. We strive to push evidence based medicine with no bias to help you obtain all the important information. You should always follow your protocols that have been set in place. And with everything in medicine, it all comes with baby steps.
–Scopeducation Team (Matt)
References
ECG Weekly posts
Farkas, Josh. “Hyperkalemia.” EMCrit Project, 4 Nov. 2019, emcrit.org/ibcc/hyperkalemia/.
“Kayexalate (Sodium Polystyrene): Uses, Dosage, Side Effects, Interactions, Warning.” RxList, RxList, 10 Aug. 2017, http://www.rxlist.com/kayexalate-drug.htm#indications.
Misch, Michael. “Crit Cases: Massive TCA Overdose: EM Cases.” Edited by Anton Helman, Emergency Medicine Cases, 11 Nov. 2019, emergencymedicinecases.com/critcases-massive-tca-overdose/.

5 Comments.
Thanks alot for yor easy ,Simple and amazing way of sharing knowledge, god plessed you .
Before I afraid and dislikes ECG ,but you made me understand and start loving it ,thank you from the deepest area of my heart
We are glad you loved it! Means a lot to us. ECGs can be very scary at first but that’s why we try to make them easy!
Very useful tips to safe patients life .
I will be very grateful if you kindly help me how to sign up .so that i get the lattest updates more frequently to improve my knowladge..
We post every week! We have a Twitter, Facebook page, and a YouTube page. We post on twitter and Facebook every time we have a new post. Below are the links. We are glad you like the page!
https://m.facebook.com/SCOPEeducation20/
https://mobile.twitter.com/scopeducation
https://m.youtube.com/channel/UCQOKy7ztXqUb1kRQTqxzgVw
Thanks from the deepest part of my heart, for the rasy , Simple and amazing way of transferring the knowledge,before i afraid and dislikes ECG .