
Is This a STEMI? ECG Changes in TBI and Increased ICP Patients
For those who wish to watch on YouTube: When it…

So when you first start studying medicine, you try as hard as you can to basically remember the waterfall of information thrown at you without caring about the big question of WHY. Always remember that the body will try to compensate in deficit area in order to remain in that happy state of equilibrium.

Knowing WHY things are occurring will greatly improve your competency and will allow you to provide better care for your patients.
In school, we were all introduced to Cushing’s Triad (Cushing’s Reflex). Cushing’s Triad occurs when there is increased intracranial pressure (ICP), which results in irregular breathing, hypertension, and bradycardia. So let us kick this thing off with a scenario.
A 40 year old male was assaulted with a metal bat. When you make contact, bystanders say he was hit in the head and is confused. Patient admits to ETOH. He has a GCS of 14 (E4V4M6). You gather the story and he lets you obtain some vitals. You are playing with two different ideas:
He takes no medications and is fairly healthy looking. He denies any hypertension. Your first blood pressure is 205/145. Pulse is regular and shows a sinus tachycardia on the 12 lead. Pt has regular respirations at a rate of 18 with no adventitious lung sounds noted. This should cause a bit of sphincter constriction inside of you.
Shameless plug: for those who want to learn how to see increased ICP on a 12 lead, check out the post below.
For those who wish to watch on YouTube: When it…
You decide to transport the patient to the local Level 1 Trauma Center in your region and during transport, the patient becomes unresponsive and his heart rate slowly starts to decline to the 60s. At the hospital, the patient has a GCS of 3, has a BP of 230/130, HR in the 30s, and breathing is noted to be irregular. It is safe to assume that the “two beers” was not to the cause. So why did the patient start exhibiting the vital signs of Cushing’s Triad?
I just wanted to address some other important information before we go too in-depth. Some of the signs of increased ICP can be confusion, loss of consciousness, delayed pupil response, “blown pupil,” headache, vomiting, posturing (decorticate/decerebrate). The two I want to hit on briefly is vomiting and “blown pupil”.
I was taught in school that it’s not IF these patients vomit, but rather WHEN these patients vomit. So be aware of that. Just some things I have noticed and confirmed throughout my time in medicine. The reason for this is because there is an increase in pressure. The brain will shift down towards the foramen magnum (towards the location of the pons and medulla oblongata). Please note that it is a common misconception that the brain herniates through the foramen magnum but that is not the case, it puts pressure on the Tentorium Incisura. In that region, there is the Vagus nerve that juts out. This will cause pressure on the Vagus which will cause it to become irritated. It is important to know the Vagus Nerve is parasympathetic.
The Vagus nerve goes off towards the heart, lungs, and GI tract and when it is stimulated by the pressure, it will overload the signals to the stomach which will induce vomiting. This will be noted as projectile vomiting.
For the pupils, we all have been told that increased ICP causes the “blown pupil”. But we want to know WHY.
This occurs due to papilledema which is in simple terms is swelling of the optic nerve. Below is a picture of the structures to help you further understand the topic.
As the ICP increases, the arterial vessel pressure in the eye seems to be okay. Where we have issues, is in the venous area. The blood is able to enter into the orbital region, but has issues with draining out through the venous side. This will cause the pupil to enlarge and become dilated. Eventually it will be refractory to light. Not trying to go too far into the rabbit hole, just some patho of WHY this occurs.
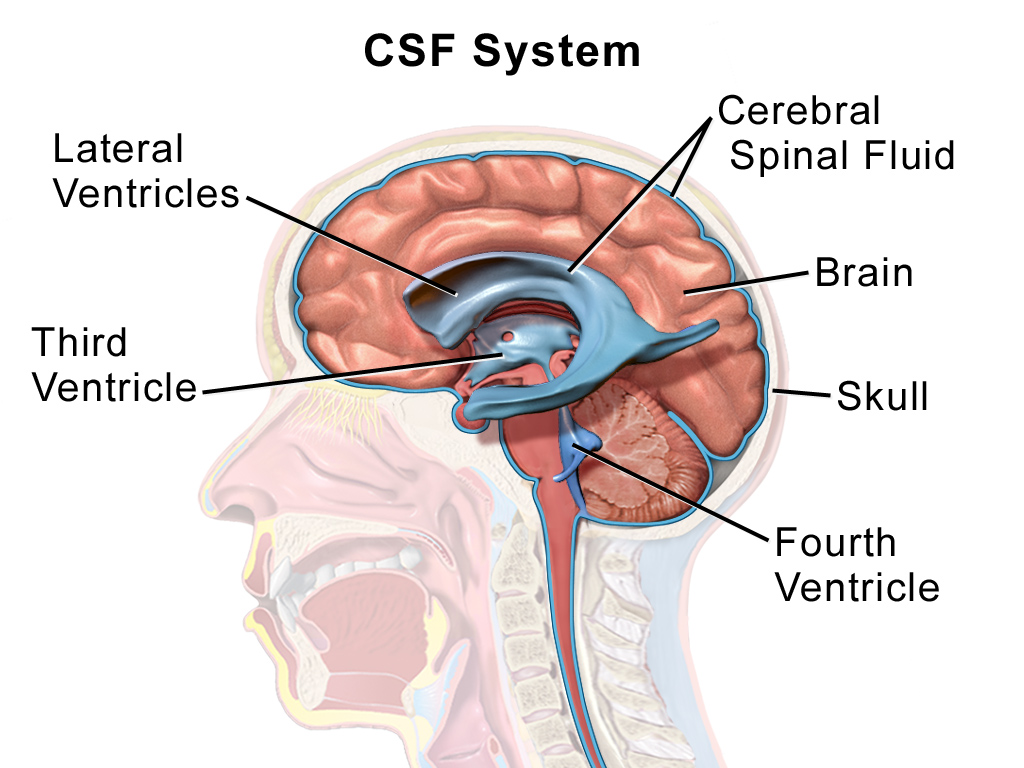
The Anatomy of the Brain
Before we get into the triad we need to understand a little bit of the brain. The brain is a spongy tissue that is enclosed inside of the skull. Surrounding the brain is a cushion called cerebral spinal fluid (CSF).
You can determine how well the brain is being perfused by calculating the cerebral perfusion pressure (CPP), which is the mean arterial pressure (MAP)- ICP. The normal CPP is usually between 60-80 mmHg. The normal ICP is between 5-15 mmHg. So based off of the formula, if ICP increases, there will be a decrease in CPP. The decrease in CPP means there is cerebral ischemia. On a bit of a side note, MAP is always the best non-invasive pressure reading to use. Below the pecking order:
For clarification check out this post:
We all have ICP. When the ICP increases, it can result in devastating patient outcomes. The skull is solid bone so when pressure builds up, the only place for the brain to go is down and put pressure on the Tentorium Incisura.
Monro-Kellie Doctrine – The sum of volumes of brain, CSF, and intracranial blood is constant. An increase in one should cause a decrease in one or both of the remaining two.
Patho of BP
This is generally the first stage of increased ICP. When there is hypoperfusion to the brain, the sympathetic (fight or flight) system is activated. When the sympathetic nervous system is activated, there will be an increase in the amount of alpha-1 adrenergic catecholamines which will of course cause vasoconstriction to increase the CPP. This vasoconstriction will cause hypertension. The catecholamines will also increase the HR in the patient by acting on the Beta-1 receptors as well. This will cause a widening in pulse pressures. I know I just mentioned previously that the Cushing’s Triad is hypertension, BRADYCARDIA, and irregular breathing.
And for those who are interested in the various receptors, here is an image that will hopefully break it down for you.
Patho of HR
So the patient is hypertensive. Why is that a problem for our heart rate? Well there is a Law we should be familiar with. Marey’s Law simply says that the heart rate and BP are inversely correlated. So if you are tachycardic, you should be hypotensive and vice versa. When you become rapidly hypertensive, the baroreceptors in the aortic arch will become stimulated due to the increased tension in the artery wall. This causes a chain reaction that impacts the HR. To put it simply, the baroreceptors send signals to a part of the medulla oblongata called the vasomotor center (VMC). The VMC will sense the increased activity from the baroreceptors and will squash your sympathetic drive and increase the vagal tone to the SA node using the neurotransmitter acetylcholine. The acetylcholine causes the decrease in the SA node to counteract the rapid spike in BP which results in bradycardia. As mentioned before, the increased ICP can put pressure on the Vagus nerve directly which can cause the bradycardia on the heart. See? Told you we would get to the bradycardia.
Patho of Respirations
So you now have your hypertension and bradycardia. So only the irregular breathing is left. Let’s take a glance at Biot’s and Cheyne-Stokes respirations.
Below is a video which includes different respiratory patterns. Hearing and visualizing will hopefully aid in developing a better overall understanding.
As the ICP increases, the brain will herniate through the Tentorium Incisura. This causes problems because the brainstem is the drive for our most basic vital signs. The two areas for respiratory control are the Medulla Oblongata (causes the breathing) and the Pons (rate of breathing). Inside of the Medulla, there are two areas that stimulate breathing.
To complicate things more, inside of the pons there are two areas as well that affect the rate:
When the brain herniates, the pressure on the medulla and pons will cause the irregular breathing we noted before.
Treatment
Now that we know the patho of Cushing’s triad hopefully we can agree that it is amazing… But it means nothing if we can’t implement the proper treatment.
Conclusion
This is for some broad info on the patho and treatment of increased ICP. TBI is not the only cause of ICP so be aware of the many other causes. Hopefully this post made this topic a little easier to understand. I tried to implement some prehospital, hospital, and critical care into this to reach a broader audience.
This site is meant to be used for educational use only. We strive to push evidence based medicine with no bias to help you obtain all the important information. You should always follow your protocols that have been set in place.
Follow our social media to stay updated!
https://m.facebook.com/SCOPEeducation20/
https://twitter.com/scopeducation?lang=en
-Scopeducation Team (Matt)
References
Armstrong, M. (2020, August 22). Physiology, Baroreceptors. Retrieved December 20, 2020, from https://www.ncbi.nlm.nih.gov/books/NBK538172/
Dinallo, S. (2020, May 24). Cushing Reflex. Retrieved December 20, 2020, from https://www.ncbi.nlm.nih.gov/books/NBK549801/
Elevated ICP: Hyperventilation. (n.d.). Retrieved December 20, 2020, from https://www.openanesthesia.org/elevated_icp_hyperventilation/
Kawahara, N., Ono, K., Sasaki, M., Tsutsumi, H., Aruga, T., Mii, K., . . . Takakura, K. (n.d.). [The effects of increased intracranial pressure on respiratory functions in clinical setting]. Retrieved December 20, 2020, from https://pubmed.ncbi.nlm.nih.gov/6466502/
Majdan, M., Mauritz, W., Wilbacher, I., Brazinova, A., Rusnak, M., & Leitgeb, J. (2013, January 1). Barbiturates use and its effects in patients with severe traumatic brain injury in five European countries. Retrieved December 20, 2020, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3530930/
Munakomi, S. (2020, November 17). Brain Herniation. Retrieved December 20, 2020, from https://www.ncbi.nlm.nih.gov/books/NBK542246/
Paravati, S. (2020, July 26). Physiology, Catecholamines. Retrieved December 20, 2020, from https://www.ncbi.nlm.nih.gov/books/NBK507716/
Whited, L. (2020, April 29). Abnormal Respirations. Retrieved December 20, 2020, from https://www.ncbi.nlm.nih.gov/books/NBK470309/






1 Comment.
Great article, thank you Matt!